Anterior Knee Pain (AKP), Alignment and Injury in Dance | Dr. Victor K. Lin
Anterior (front) knee pain is the most common knee injury in dancers. It is a repetitive stress in-jury (RSI) that afflicts up to 33% of dancers. Because it is often difficult to manage, it is the subject of considerable research—which is showing that the problem may not be in your knee, but in the rest of your body.
AKP - What is it?
AKP is usually insidious in onset and progressive in nature. It starts with crepitus (grating, popping) and progresses to stiffness, catching, pain and swelling. It can be provoked by new choreogra-phy, raked stages, new shoes, or an abrupt change in dance schedule. Movements such as grand plié/squats (knee flex/extend), and jump/landings increase risk.
The Usual Suspect
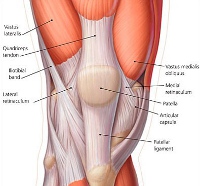
Traditional thinking in the sports medicine field is that AKP is often due to patellar-femoral syndrome: a condition where the kneecap does not track correctly in its canal (the trochlear groove). This is attributed to tightness in the iliotibial band (ITB) muscles and/or weakness of the inner quadriceps muscle (the vastus medialis obliquus or VMO).


Treatment after relative rest is vigorous stretching of the ITB and strengthening of the VMO. The key to stretching the ITB is stretching its two components—the tensor fascia lata (TFL) and the gluteus maximus. Both must be stretched. Strengthening the VMO involves shallow, slow lunges in multiple directions, or squeezing a ball between the knees with the injured leg straight out.

Biomechanical Research
Research regarding this injury is showing that dancers with this injury frequently have difficulties elsewhere. The Harkness Center for Dance Injuries in New York showed a significant correlation between deficient torso strength, torso proprioception (position sense), hip weakness, hip tightness and knee injury, particularly AKP. Conversely, they found that dancers with good torso, pelvis/hip strength, flexibility, and coordination had dramatically decreased incidence of knee injury/pain.
Similarly, dancers with ankle injuries had deficits in hip strength and coordination, and athletes with these deficits were found to have an increased chance of ankle injury.
“Knock-knees” (known in the sports medicine field as increased genu valgus or increased “Q-angle”), particularly in the female athlete, are frequently associated with knee injuries. But what is less-emphasized is the role of proper alignment in injury preven-tion. The body is a chain of linkages, and the position of one affects the next.

In many cases, knock-knees are due to inward rotation of the thighs at the hip. This leads to a compensatory outward rotation torque effect on the lower leg, and predisposes to a flat foot in athletic activities, particularly with movements in dance. Dancers with this condition frequently compensate by placing their feet in the proper position for turnout, then push up from the floor, torquing their lower leg, putting extra stress on the knee joint.

The chain can also work in reverse. Flat feet can force the lower leg to compensate with increased outward rotation, putting strain on the knee. Decreased ankle movement in bending and straightening (dorsiflexion and plantarflexion, respectively) due to tight calves or a prior ankle injury puts strain on the foot towards increased flatness and subsequent rotation stress on the lower leg and then the knee.
Additionally, biomechanical research is also recognizing the importance of the hamstring muscle in controlling lower leg rotation with athletic activity. A strong and coordinated hamstring is critical to decreasing the risk of knee injury.
The increased incidence of anterior cruciate ligament (ACL) injuries in female athletes, particularly in sports like soccer, led to a similar analysis in dancers. The ACL is one of the four critical stabilizing ligaments in the knee, and an injury to it can be devastating, requiring surgical repair and/or 9-12 months of rehabilitation.

Interestingly, the incidence of ACL injury in female ballerinas is relatively low. At the Harkness Center for Dance Injuries, research showed that the jump training young dancers received in traditional ballet programs reduced their risk of such injuries compared to other female athletes. The emphasis on landing a jump with the balls of the feet first promotes a protective knee bend on impact. Indeed, research in female soccer players concurrently revealed that improper landing technique and a quadriceps/hamstring strength imbalance contributed significantly to their higher incidence of ACL injuries versus males. It is now recommended that female athletes learn how to land from a jump correctly (bending the knees to absorb the shock of landing) and undergo directed hamstring strengthening as part of a standard preventative program.
ACL injuries can and do occur in dancers—they are just at lower risk than other female athletes. Research has also found that the incidence of dance injuries is dramatically higher towards the end of the dance season, or towards the end of the day—that is, when the dancer is tired.
Conclusions
It is critical for the dancer to regain flexibility, strength, proprioception, and proper technique during the rehabilitation phase of recovering from every injury. Failure to do so, even if the injury feels like it has recovered, may result in recurrence of that injury, or compensatory injury elsewhere along the body's kinetic chain.
Finally, recurrent injury is a red flag. It either means the dancer is not taking the time to recover fully and/or properly, or that the dancer is compensating for poor biomechanics. Biomechanical deficits due to natural anatomy are difficult to correct, but can be modified somewhat with stretching and strengthening (“body-shaping”), alignment optimizing, and orthotics or taping. Biomechanical deficits due to faulty technique should be investigated and corrected. Both approaches should be undertaken with the help of a qualified dance instructor and, if necessary, a health care provider familiar with dance technique.
Links:
1. “Patellofemoral Exercises” Kaiser Permanente, Physical Therapy Department, on rehabilitating patellar-femoral syndrome
References:
1. “Principles of Dance Medicine, Clinical Management of the Dancer
Patient”, an Educational Conference at the Harkness Center for Dance
Injuries, July, 2010.
2. Dance Injury & Prevention, 3rd Edition by Justin Howse, MD. Routledge
Publications.
3. Preventing Dance Injuries, 2nd Edition by Ruth Solomon, John Solomon, and
Sandra Cerney Minton. Human Kinetics, 2005.
Photo Credits:
1. Figure 2 photo rights purchased from istockphoto.com
2. Figure 3 photo by lululemon at Flicr.com under the terms of their
Attribution License
3. Figure 4 photo by mkd from Flickr.com under the terms of their Attribution
License
4. Figure 6 ABOVE photo by Pixel ;-) from CommonsWiki under the terms of the
GNU Free Documentation License
5. Figure 6 BELOW photo from imageshack.us under their Terms of Service
6. Figure 7 rights purchased from istockphoto.com